Transcrestal Sinus Floor Elevation
Pdf Transcrestal Sinus Floor Elevation With Osteotomes Simplified Technique And Management Of Various Scenarios
Http Onlinelibrary Wiley Com Doi 10 1111 Prd 12165 Pdf
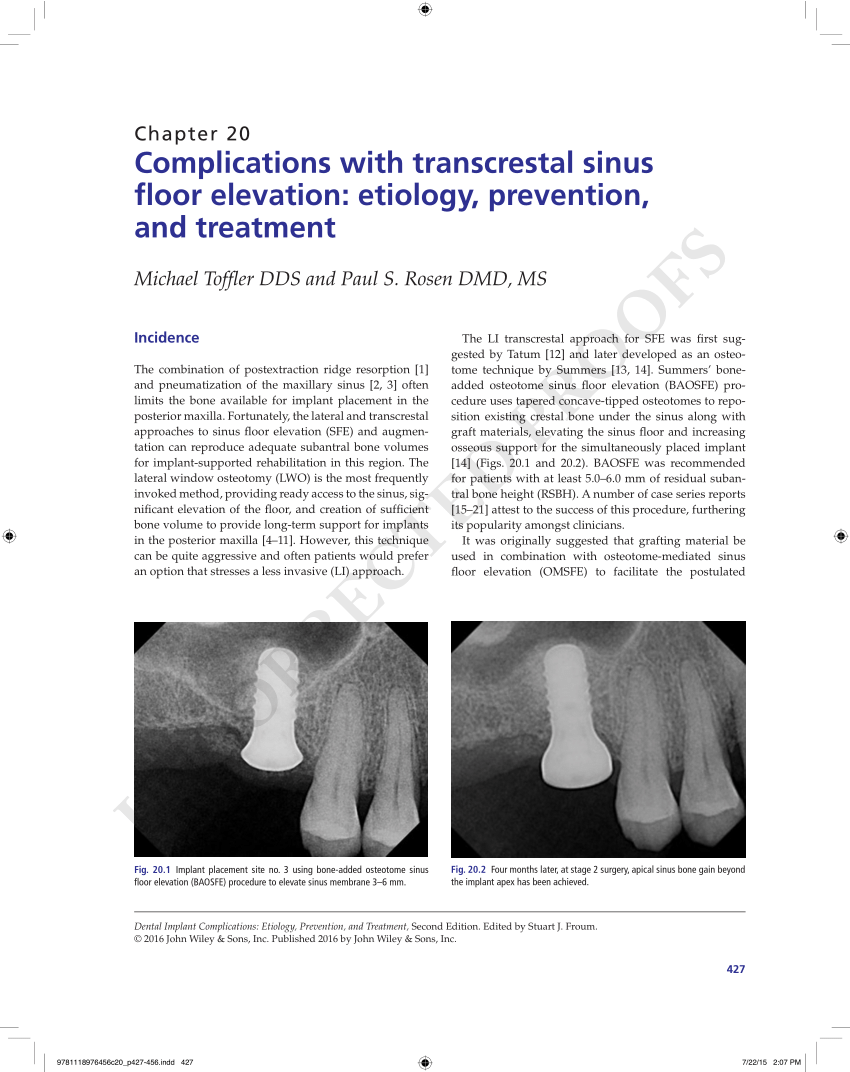
Pdf Complications With Transcrestal Sinus Floor Elevation Etiology Prevention And Treatment

Transcrestal Sinus Floor Elevation With Osteotomes Simplified Technique And Management Of Various Scenarios Compendium Of Continuing Education In Dentistry May 2011 Compendium Cdeworld

View Image
Maxillary Sinus Floor Elevation
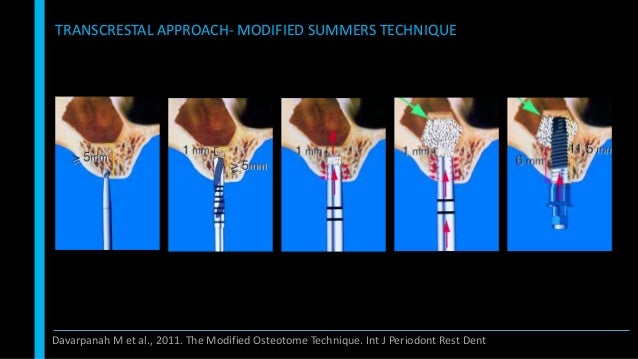
The technique is based on the use of specially designed drills and osteotomes.
Transcrestal sinus floor elevation.
.jpg)
Figure 3

Pdf Classification Of Sinus Membrane Perforations Occurring During Transcrestal Sinus Floor Elevation And Related Treatment Semantic Scholar
Pdf Minimally Invasive Transcrestal Sinus Floor Elevation With Deproteinized Bovine Bone Or B Tricalcium Phosphate A Multicenter Double Blind Randomized Controlled Clinical Trial
Sinus Floor Elevation

A Minimally Invasive Technique For Transcrestal Sinus Floor Elevation Dt Science
Pdf Sinus Floor Elevation Using Osteotomes A Systematic Review And Meta Analysis

Pdf The Endoscopically Controlled Osteotome Sinus Floor Elevation A Preliminary Prospective Study Semantic Scholar

Iti Treatment Guide Volume 5 Sinus Floor Elevation Procedures
The Hydraulic Lifter Of The Crestal Approach Sinus Kit It Is Connected Download Scientific Diagram

The Percrestal Sinuslift From Illusion To Reality 9781850972228 Medicine Health Science Books Amazon Com
Pdf The Incidence Of Maxillary Sinus Membrane Perforation During Endoscopically Assessed Crestal Sinus Floor Elevation A Pilot Study

New Bone Formation After Transcrestal Sinus Floor Elevation Was Influenced By Sinus Cavity Dimensions A Prospective Histologic And Histomorphometric Study Megagen Implant

Summers Modified Diagrams Illustrating Sinus Floor Upfracture Using Download Scientific Diagram
Pdf Severe Bleeding After Sinus Floor Elevation Using The Transcrestal Technique A Case Report
Inlay Osteotome Sinus Floor Elevation With Concentrated Growth Factor Application And Simultaneous Short Implant Placement In Severely Atrophic Maxilla Topic Of Research Paper In Medical Engineering Download Scholarly Article Pdf And

Pdf Short 6 Mm Dental Implants Versus Sinus Floor Elevation And Placement Of Longer 10 Mm Dental Implants A Randomized Controlled Trial With A 3 Year Follow Up

Internal Sinus Lift Youtube
Pdf Osteotome Mediated Sinus Floor Elevation A Clinical Report

Sinus Floor Elevation Procedures To Enable Implant Placement And Integration Techniques Biological Aspects And Clinical Outcomes Semantic Scholar
Source : pinterest.com
